Among community older adults (age 65-75) and in preceding one week
Depression and Anxiety are two most common mood disorders in older adults
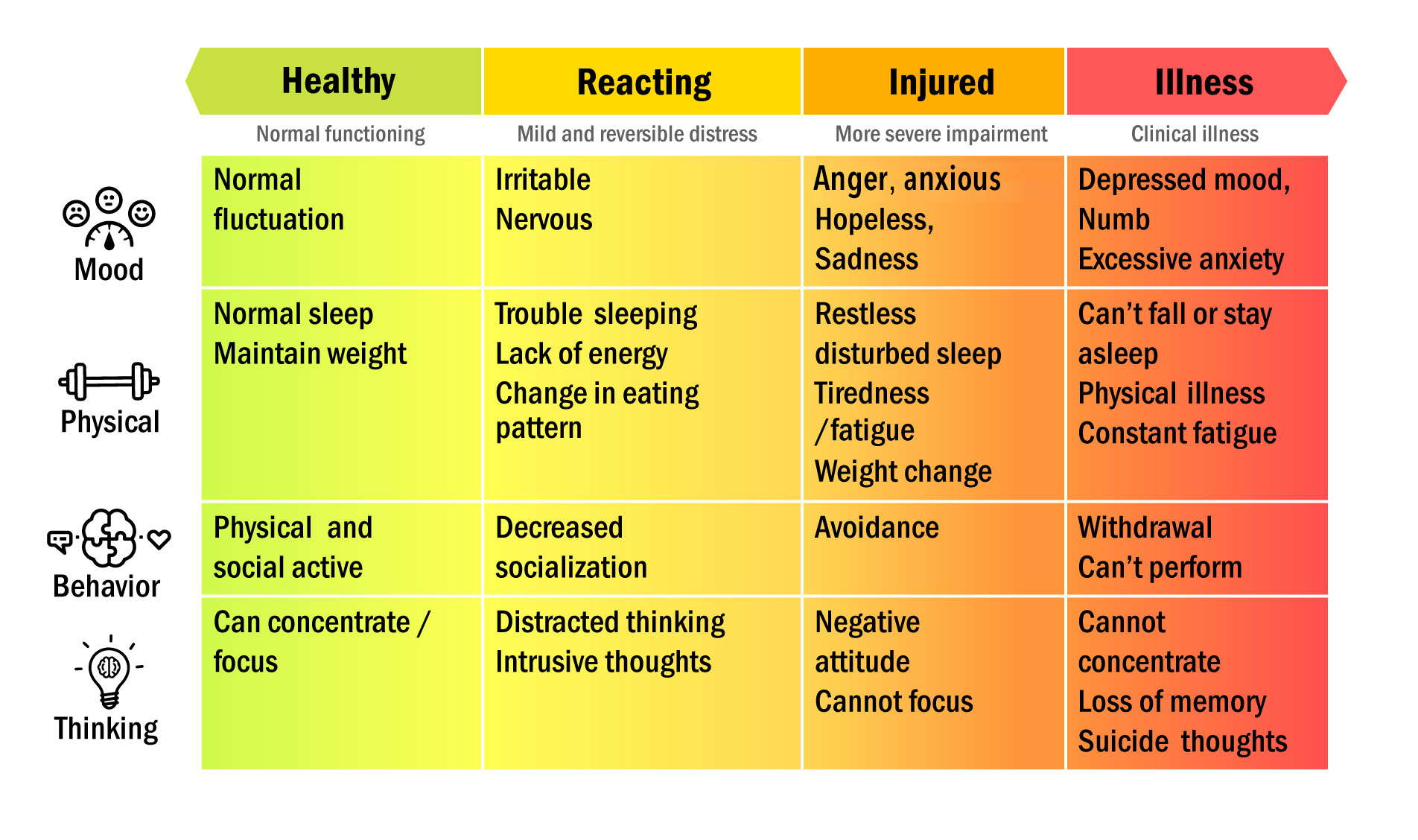
However, remember from the “Mental Health Continuum Model”
- Continuum from healthy to illness
- Depressive episode: 4.7%
- Using depressed mood as example,
NOT all “depressed mood” = "depression”
Depression is considered to exist on a continuum from normal sadness (mood symptom) to pathological severe depression (disorder)
Why are elderly so prone to have mood problem ?
Factors affecting psychological health
Chronic disease
Physical impairment with functional limitations
Pain (both physical limitation or the feeling of not so able)
Psycho-social elements: Grief, loneliness or major life events including relocation (going to old age home), loss of dignity and respect
Side effects of medications
Personality, Coping skills and Social Support
Older adults may have…
Distress and sense of helplessness from functional impairment / communication challenges
Adjustment difficulty after retirement: lack of life goal / financial independence
Social isolation and feelings of out of touch
Loss of confidence and self-worth
Sense of loneliness
Going back to Question 1: Do you think Mr O has depression?
Depression (for adults)
It is a broad and heterogeneous diagnosis
Distinction should be made between “depressive mood” (symptom) versus “depressive disorder”
The WHO International Classification of Diagnosis version 10 (ICD-10) or Diagnostic Statistical version V (DSM-V) give reference guidelines to the diagnosis on mood disorders
Diagnostic reference to Depression (not diagnostic criteria)
Depressive Disorder (ICD-10)
- At least 2 out of 3 (low mood, loss of interests / pleasure, loss of energy) symptoms plus
- Others (reduced concentration, reduced self-esteem, guilt feeling, pessimistic, idea or act of self harm, disturbed sleep, reduced appetite)
- Present for at least 2 weeks
- Severity (mild, moderate, severe) depends on clinical assessment on severity of each and total number of symptoms
Diagnostic reference to Depression
DSM-V for Major Depressive Disorder (at least 5/9 for at least 2 weeks)
- Core Symptoms:
Depressed mood AND / OR
Reduced interest / pleasure
- Somatic Symptoms:
Change in appetite
Change in sleep pattern
Reduce energy level
Psychomotor agitation / retardation
- Cognitive Symptoms
Poor concentration
Inappropriate guilt
Tight death, suicide
Depressive mood versus Depressive disorder
Subthreshold depressive symptom
- One symptom of depression but with insufficient others symptoms / functional impairment to meet criteria for full diagnosis (of disorder)
A PHQ-2 score of 3 or more has sensitivity of 84% in detecting depression
A GDS-4 score of 2 or more has 60-76% sensitivity in detecting depression
Reference source from : Hong Kong Reference Framework for Preventive Care for Older Adults in Primary Care Settings - Module on Common Mental Health Problems in Older Adults 2019
Is it likely to be depression?
Detailed assessment with PHQ-9 or GDS-15 is recommended if PHQ-2≥3 or GDS-4≥2
Reference source from : Hong Kong Reference Framework for Preventive Care for Older Adults in Primary Care Settings - Module on Common Mental Health Problems in Older Adults 2019
Anything more serious?
Assess Red Flag
- Self Harm: any thought or planned act
- Psychosis / Mania: hallucination / false belief
Summary of Chapter 1
Mood issue is a continuum from normal emotional response to clinical disorder
- Depressed mood ≠ Depressive disorder
Two questions to ask
- Is it likely depressive mood or depressive disorder?
- Is there any suggestion that the person may endanger oneself or others?
Depressive mood versus Depressive disorder
Two steps approach
- Preliminary Screening → Detail assessment
Preliminary Screening
- Single question: “ Over the past 2 weeks, how often have you felt down, depressed, or hopeless?” (PHQ-2) OR
- Geriatric Depression Scale - 4 question version (GDS-4)
Detailed assessment
- PHQ-9 or GDS-15 is recommended if PHQ-2 ≥ 3 or GDS-4 ≥ 2
Refer if PHQ-9 ≥ 10, or GDS-15 ≥ 8
Suggestions of danger
Red Flag feature
- Self Harm: any thought or planned act
- Psychosis / Mania: hallucination / false be
Refer if yes
- End of Chapter 1-
课程第二週
MOOC 7 Chapter 2
Let's recall...
What you expect to understand…
Mood issue is a continuum from normal emotional response to clinical disorder
Common mood issues in old and how the same condition differs between older adults and the younger counterpart
The multi-dimensional aspects on emotion and mood
Preventive measures
Common assessment / screening tools
What you can do if you suspect the elder has mood issue
Case study Story of Mr O (2)
The story continue...
Wait...
Mr O has a number of somatic complaints, and anxiety is more common than depressive episode (see Chapter 1), can he have anxiety or other medical diseases?
Anxiety Disorder in older adults
Anxiety, depressive episode and the combinations are the commonest
- Generalized anxiety disorder (GAD) and mixed anxiety and depressive disorder are the two commonest form
- Any common mental disorder: 11.2%
- Depressive episode: 4.7%
- Generalized anxiety disorder: 5.5%
- Mixed anxiety and depressive disorder: 3.6%
- Other anxiety disorder: 1.24%
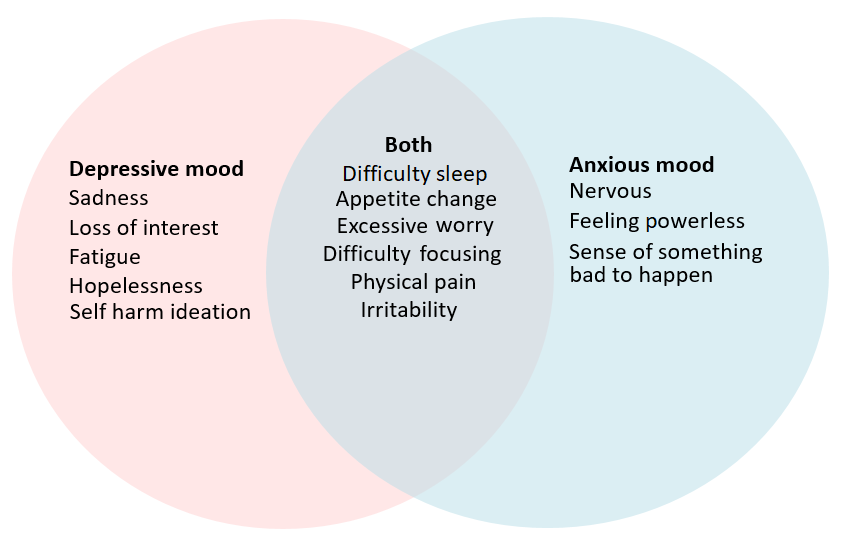
There are large overlap on manifestations between depressive mood and anxiety as they share common risk factors
- cross reference slide:
Chapter 1: Low Mood - Factors affecting psychological health
The overlap between depression and anxiety
Diagnostic reference to GAD in adult (ICD-10)
Generalized Anxiety Disorder (GAD) is characterized by generalized and persistent anxiety (most days for at least several weeks) in any environmental circumstances
- Somatic symptoms from chest (eg. fear of choking, chest discomfort) and abdomen (eg. churning in stomach)
How older person differ?
Older adults commonly have the following symptoms
- More somatic symptoms
- Excessive uncontrollable worry / anxiety
- Edginess, nervousness or restlessness
- Chronic fatigue or tiring out easily
- More irritable or agitated
- Poor quality of sleep or difficulty falling / stay asleep
- Tense muscle
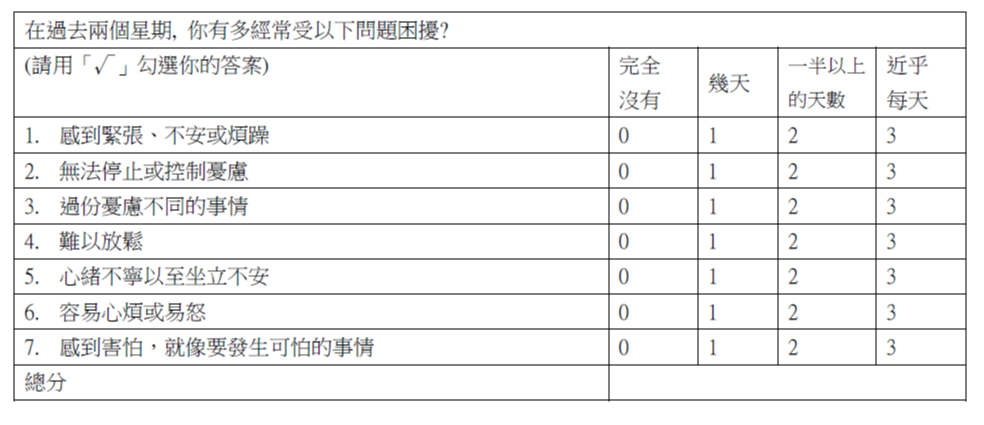
How to screen for GAD in older adults?
The GAD-7 Scale can be used a rough guide for screening
Scores of 5, 10, 15 are used as cutoff for mild, moderate and severe GAD
Reference source from : Hong Kong Reference Framework for Preventive Care for Older Adults in Primary Care Settings - Module on Common Mental Health Problems in Older Adults
Case study - Story of Mr.O
Let’s also recall Mr O had
- Low energy state (more tired, social withdraw, loss of appetite)
- Somatic complaints (generalized aches and pain)
- Poor sleep
- On and off in past few months but not persistent
PHQ-9 scored 5/30 and GDS-15 at 5/15
There is no red flag feature
A GAD-7 was also performed on Mr.O of which he scored 4/21
Yes .. You need to explore concerns from Mr O. How to do so?
You need to
- Built rapport: you are concerned about him
- Ask if he has any concern / worry about himself
- Ask about psycho-social stress:
Recent stress and coping strategy
Daily functioning
Role changes (care-giver strain)
Ask about his physical functioning
Case study - Story of Mr O (3)
Discussion
Mr O is likely to have subthreshold depressive symptom. The main stressor likely from coping with wife who has dementia (care-giver strain)
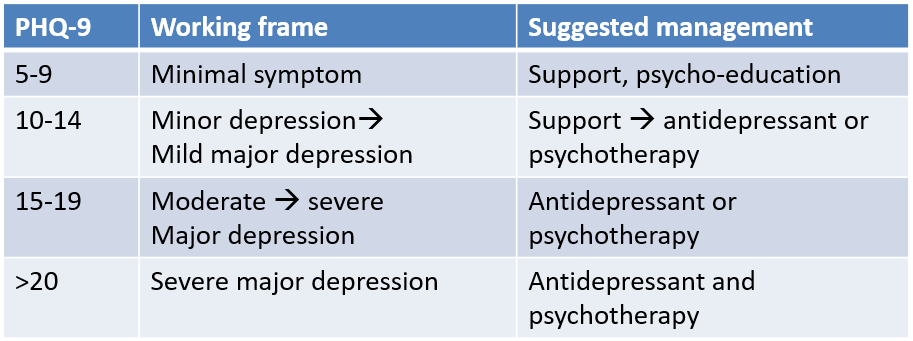
A rough guide on management strategy is provided by PHQ-9
Summary of Chapter 2
About 10% of local older persons have anxiety related issues
Sleep problem, appetite change, excessive worry, fatigue, physical pain are common symptoms for both anxiety or depressive issue
The GAD-7 is a useful tool for assessment
To address anxiety and depressive issue, it is essential to explore and identify the stressors for psychosocial support
-End of Chapter 2-
课程第三週
MOOC 7 Chapter 3
Let's recall...
Recall on Mr O
Mrs O had dementia and was getting worse
Mr O was main caregiver to Mrs O
- Felt tired in coping
- Worried on her worsening and he could not cope
- Felt alone by himself
Mr O was likely to have depressive episode from caregiver strain
Understanding Caregiver Strain
Many older persons who suffer chronic illnesses require constant care from their family members
Caregivers stretch themselves too far in the care-giving roles and ignore their own needs
A mental status called “Burnout” would emerge if caregivers could not manage their stress properly
Symptoms of “Burnout”
Physical: Feeling fatigue & sick, and ignoring time for taking rest and meals
What family /friends can do with a depressed older adults
Be with them but NOT to disparage their feeling
- Talk and listen with appropriate assurance
- Point out realities and offer hope
Encourage and assist in seeking help
Find out local support group and attend meeting with them whenever possible
Alert on severe depression (and cues on active attempt of suicide)
Is drug treatment good to older adults?
You learnt for previous slides that antidepressant may be used in major depression, yet need to balance between risk and benefit. Overall, older adults are prone to have the following side effects (True / False)
(A) Increase falls?
(B) Increase cardiac arrhythmia?
(C) Accelerate cognitive decline?
(D) Upper gastrointestinal bleeding?
Feedback of "Is drug treatment good to older adults?"
Any False / True:
Though different drug class or different drug within same class may have different side effects profile, older adults are more prone to side effects of individual drug overall.
Besides, older adults tend to be on multiple drugs because of multiple pre-existing diseases. Drug-drug (prescribed or over-the –counter supplements) interactions may occur leading to predictable or unpredictable that side effects.
Pharmacological intervention should always be judged on balance of risk / benefit and among different treatment options.
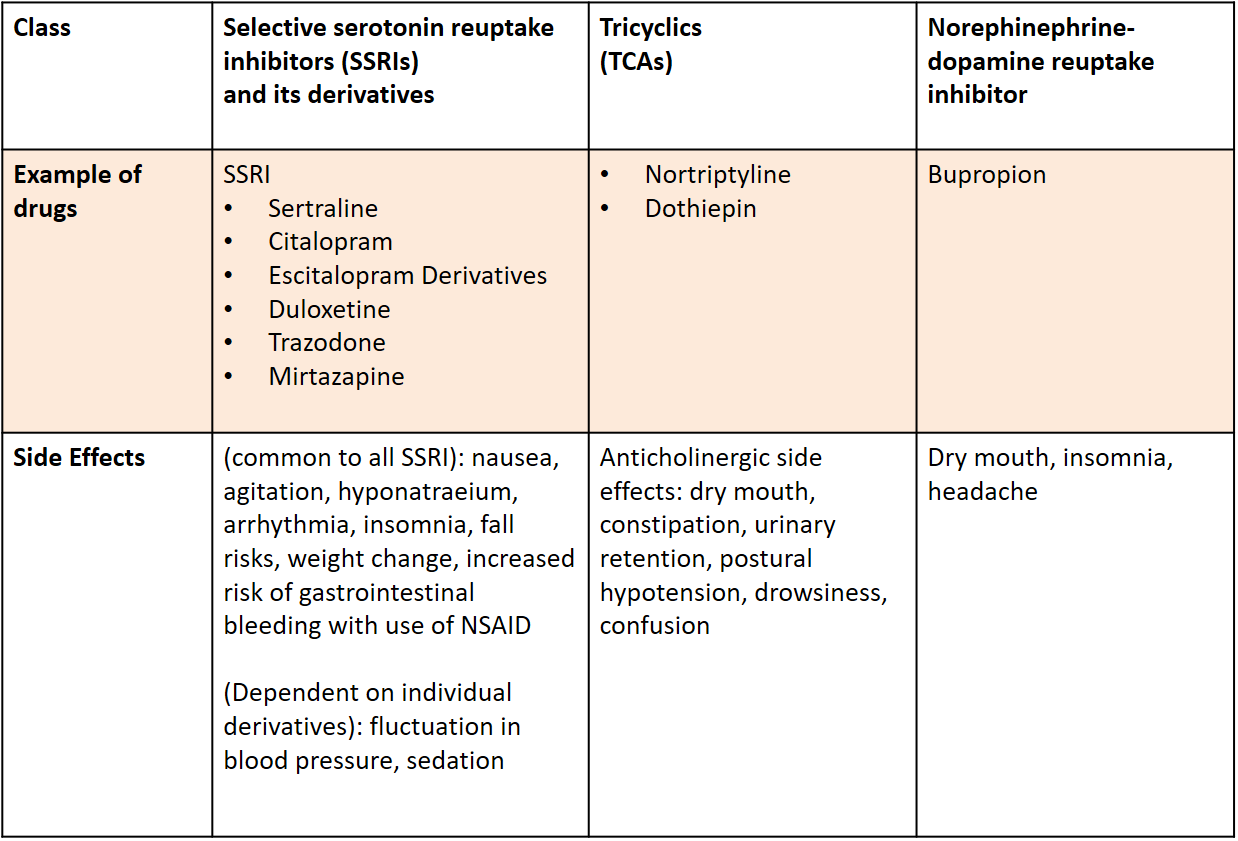
Common antidepressant drugs and side effects
margin-top:25px;margin-bottom:15px;
The Story of Mr O (4)
End of the story
His sleep, appetite and energy level recovered over 3 months
Overview on mood and mental problems in older adults
Older adults are prone to have mental / mood problems because of
Reference source from : Hong Kong Reference Framework for Preventive Care for Older Adults in Primary Care Settings - Module on Common Mental Health Problems in Older Adults 2019
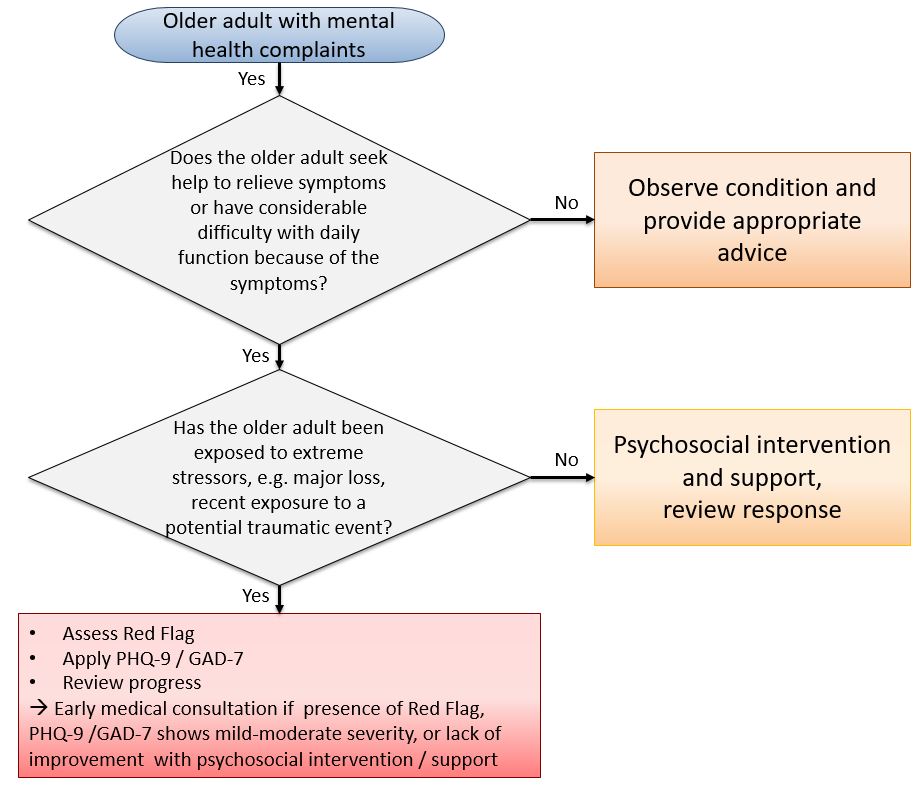
Management of mild mental health complaints
Pyscho-social intervention
- Acknowledge symptoms
- Ask for their own explanation of the cause of symptoms and elicit their concerns
- Discuss potential links between the person’s emotions/stress and symptoms
- Promote self-care: reduce stress, strengthen social support, maintain healthy lifestyle and promote functioning in daily activities
Support and give advice to the caregivers
Monitor of progress
Report to family doctor at next scheduled follow up who may
- Review if any investigation is necessary
- Avoid ordering more investigations than is necessary
- Communicate with patient about the normal clinical and test findings and reassure that no serious disease has been identified
- Consider if antidepressant or anxiolytic drugs is needed (usually not necessary)
Summary of Chapter 3
Older adults are prone to have mental / mood problems because of
Reference source from : Hong Kong Reference Framework for Preventive Care for Older Adults in Primary Care Settings - Module on Common Mental Health Problems in Older Adults 2019
Psycho-social Management
Active listening and in non-judgmental way
Allow expression of emotion and express empathy
Identify areas of concern
Guidance / psycho-education
- Give information and provide rationale
- Suggestion, guidance and advice
Strengthen social support and mobilize community support
Clark, L.A., Cuthbert, B., Lewis-Fernández, R., Narrow, W.E., Reed, G.M. (2017). Three approaches to understanding and classifying mental disorder: ICD-11, DSM-5 and the National Institute of Mental Health's Research Domain Criteria. Psychological Science in the Public Interest, 18(2), 72-145.
Stein, D.J., Szatmari, P., Gaebel, W., Berk, M., Vieta, E., Maj, M., Vries, Y.A.D., Roest, A.M., Jonge, P.D., Maercker, A., Brewin, C.R., Pike, K.M., Grilo, C.M., Fineberg, N.A., Briken, P., Cohen-Kettenis, P.T., Reed, G.M. (2020). Mental, behavioral and neurodevelopmental disorders in the ICD-11: an international perspective on key changes and controversies. BMC Medicine. 18, 21. Retrieved from https://bmcmedicine.biomedcentral.com/articles/10.1186/s12916-020-1495-2